 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| HOME >Spring 2009 - Volume 53 - Number 2 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Why Do Children Become Crown Wards and How Are They Doing? The population of children in care at Family and Children's Services has increased dramatically over the last 10 years. We found that we did not have an adequate explanation as to why so many more children were remaining in care. Consequently, in 2008, a research study was conducted that attempted to uncover the most significant factors affecting decisions to pursue Crown wardship at the agency, examined the progress of all children and youth who were currently Crown wards, and explored whether any relationship existed between the factors leading to children becoming Crown wards and how they progressed in long term care. The following is an abbreviated version of the full study. Literature Review The approach taken to the literature review was to examine any previous reviews that had been completed about how children and youth progress while in long term care. To summarize the highlights from the review, we can conclude from the literature that adults who have been in foster care often have more personal issues than the general population and do not attain similar academic levels or employment stability (Blome, 1997; Buehler, Orme, Post and Patterson, 2000; Cook-Fong, 2000; Orangewood Children's Foundation, 2001). Some of the studies also identified areas of resilience in the lives of adults formerly in foster care (McDonald, Allen, Westerfelt and Piliavin ,1996). Outcome studies of children living in long term foster care indicate the presence of significant mental health issues (Bellamy 2007; Marquis and Flynn, 2008), but we know little about the trajectory of their personal well-being over time due to the limited number of outcome studies of children while in foster care; we know that they are often not attaining satisfactory levels of academic functioning during their time in care (Trout, Hagaman, Casey, Reid and Epstein, 2008); and we know from the limited studies soliciting the views and feelings of children in care that relationships are important to them (Adair, 2007; Farruggia, S. P., Greenberger, E., Chen, C., and Heckhausen, J., 2006; Leathers, 2005). This study will attempt to expand the knowledge base about the trajectory that occurs during the course of long term placement in care and will examine how the children and youth view their well-being. In doing so, we may learn more about how to prepare these children and youth for success in their adult lives. Methods The design incorporated both a longitudinal case study approach as well as cross sectional surveys. The longitudinal case study was used to capture outcomes by assessing the functioning of the Crown wards upon entry to care and at various junctures during their time in care. The cross sectional surveys were administered to capture intermediate and/or long term outcomes after the children and youth had been in care for at least two years. 1) A file review was conducted to examine why the children in the care of the agency had become Crown wards. Affidavits, child protection service plans and the Ontario Risk Assessment Model (ORAM) (OACAS, 2000) were the primary sources of information. The intent was to develop a comprehensive analysis of the factors that resulted in Crown wardship. 3) Current well-being was also established through the Kidscreen quality of life questionnaire (Ravens-Sieberer, 2006), and the Asset Profile from the Ontario adaptation of Looking After Children (OnLAC) (Flynn, Ghazal, and Legault, 2006). Academic progress was examined by reviewing the school report cards contained in each child's file. Sampling Frame Results Table 1 shows that the sample is evenly balanced between females (46) and males (49). The three age groups (8-11 years; 12-15 years; 16-18 years) examined are also fairly balanced. The rationale for the three age groups was to isolate latency, early and mid adolescence, and late adolescence for the purpose of data analysis. A small percentage of the sample are Crown wards without access. Of those having access, it is interesting to note that 28 are visiting frequently (every 2 weeks or more). The quality of the access seems to be mostly neutral or positive as rated by the children's services workers. The number of admissions prior to Crown wardship are concerning. As is the case provincially, the number of placements after the most recent admission to care is high; 65 percent of our Crown wards have experienced 4 or more placements. The OnLAC data shows that across Ontario 81 percent of Crown wards have experienced that number of placements. Table 1
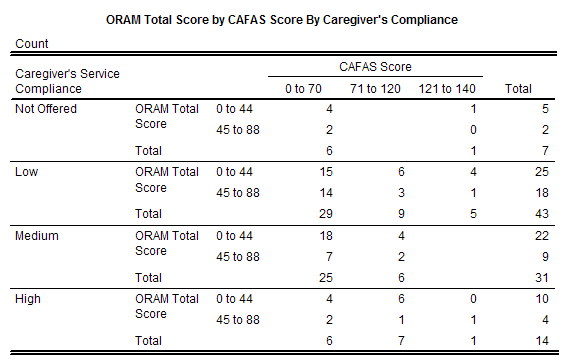
From the Eligibility Spectrum (OACAS, 1997) we learned that caregiver with a problem, caregiver/child conflict and physical maltreatment were the top three reasons for the child protection cases being open at the time children and youth were admitted to care. The most frequent parental problems found through examination of the files were, in descending order, as follows: substance abuse by the caregiver, poor parenting and household management, neglect of the child's essential needs, child behaviour, and the caregiver's mental health. The most frequent services used by parents were parental/family counseling (child-related), mental health assessment/treatment, addiction services and individual/financial counseling. Another element important to understanding why these children and youth became Crown wards involves the examination of risk assessments. All Crown wards in the study were admitted to care when the Ontario Risk Assessment Model was still the risk assessment being used in the province of Ontario. Overall risk as measured by child protection workers is placed on a 5 point Likert scale that corresponds to the following ratings: low, moderately low, intermediate, moderately high and high. The risk ratings were as follows: 2.1% at moderately low risk; 32.6% at intermediate risk; 41.1% at moderately high risk; and 24.2% at high risk. The mean overall risk rating on the 5 point scale was 3.87, almost at the moderately high level of risk. Another method, used by Leshied et al., (2003) is to sum up the numerical ratings for the 22 risk variables. The total possible score is 88. Applying that method found the mean of the total risk score to be 41 which is slightly below the mid point of the highest possible score. It is difficult to know which method most accurately measures overall risk: the first method may over-estimate risk both because it is more subjective and reflects a time period when the risk paradigm was pervasive; and the second method may under-estimate risk because it does not take into account the interaction of risk and protective factors being considered by child protection workers in their analysis. Parental service compliance was also examined. The following results were found: 7.4% of the parents were not offered a service; 45.3% had a low level of compliance with the agency's child protection service plan; 32.6% demonstrated medium compliance; and 14.7% demonstrated high compliance. A further area examined was chronicity as defined by looking at the number of admissions to care prior to Crown wardship. We defined 3 or more admissions as chronic and 1 or 2 admissions as non-chronic. We found that 25 of the cases were chronic and 70 of the cases were non-chronic. For the chronic cases, the average admission CAFAS score was 66 and for the non-chronic cases the average admission CAFAS score was 51. For 15 of the 25 chronic cases the CAFAS score was below 70, and for 10 it was above 70. Table 2 attempts to further analyze the interaction of the various factors leading to Crown wardship. The variables considered are the risk rating, the child's behavioural and mental health functioning at admission as measured by the Child and Adolescent Functional Assessment Scale, and the level of service compliance. In Table 2 the total risk score method is employed with the risk score banded into two levels; above the mid-point of the total score; and below the mid-point of the total score. Although Leshied et al. (2003) found a substantial level of inter rater reliability among child protection staff completing ORAM, we chose to rely on the cumulative risk score method as it is less prone to subjectivity than the overall risk rating selected by child protection workers. The CAFAS scores were banded into three categories: 0 to 70 (mild to moderate severity); 71 to 120 (moderate to high severity); and 121 to 240 (extreme severity). In cases for which the CAFAS score total at admission was less than 70, the risk rating was intermediate or less, and there was medium to high service compliance on the part of parents leading up to Crown wardship we posit that the necessity of Crown wardship may be questionable. Our analysis indicated that 22 cases involved situations in which Crown wardship might have been averted.
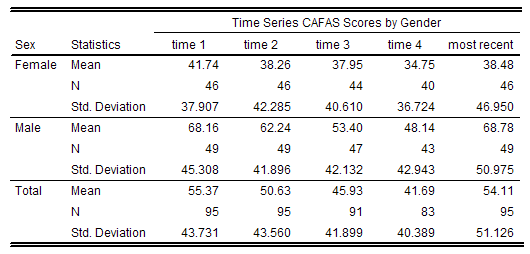
Outcomes for Crown Wards Table 3 shows time series data that illustrates how the Crown wards in the sample are progressing over time. Based on the CAFAS score results, it was found that upon admission 71% of the children and youth met the criteria of that instrument for a referral to mental health services. Males come into care with an initial CAFAS score that is higher than for females. Over the first two years in care both genders improve in their emotional and behavioural functioning; however, when the most recent CAFAS score is considered both groups drift upward and have mean scores close to their CAFAS score results at admission. Separation of the most recent CAFAS scoress into groupings based on age seems to offer an explanation for this deterioration. Specifically, the 8 to 11 year old group continues to improve by the most recent CAFAS score, the 12 to 15 year olds have the same mean scores as they did at admission, and the 16 to 17 year olds have worse scores than they did at admission. Thus the onset of adolescence may provide some insight into the trend. Various correlations between CAFAS score and other variables were found. A strong correlation was found between the total CAFAS scores and the number of placements children and youth had experienced since their last admission to care. The Pearson correlation of .48, which was significant at the .01 level indicates that a strong positive correlation exists between the number of placements and the seriousness of the CAFAS score. The most recent CAFAS total score correlated at the .01 level of significance with a number of Kidscreen dimensions which indicates that as the CAFAS scores deteriorated so did the child's perception of his/her quality of life. No correlation was found between CAFAS scores and frequency of access.
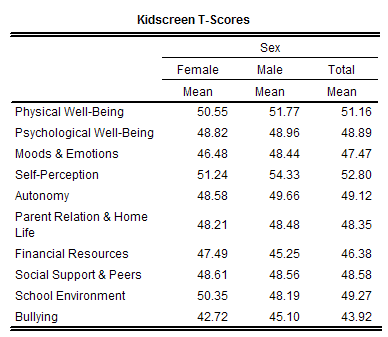
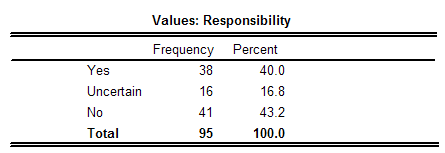
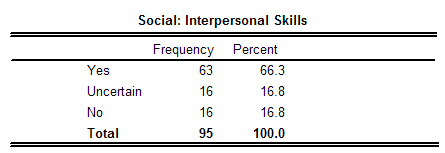
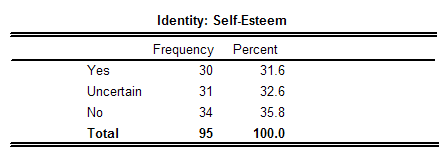
Table 4 depicts the results from Kidscreen, the tool with which Crown wards rated their quality of life. The instrument has been tested with 20,000 children and youth from the general population across 13 European countries. The mean for the general European population of children and youth, which ranges from 48 to 52, varies somewhat for each of the scales and for males and females. Female Crown wards were found to be in the normal range for five scales: physical well-being; psychological well-being; self perception; autonomy and school environment. Males were found to be in the normal range for two scales: physical well-being; and self perception. Bullying was the dimension on which they gave the poorest rating; many reported a sense of being bullied. The following provides a sense of some of the most salient responses given by the participants: a) 71.8% said that life was very or extremely enjoyable; b) 68.2% said they were very or extremely satisfied with life; c) 64.7% said they were very often or always cheerful; d) 85.9% said that they seldom or never felt that everything in their life went wrong; e) 88.3% said they seldom or never felt lonely; and f) 73% said that they were very often or always happy with the way they are. It is well established that particular assets act as protective factors for at-risk children and youth. Moreover, these assets may enable them to overcome the adversity they have encountered in their lives. Thus the asset profile from OnLAC, which helps identify the degree to which these assets are present for a child, is of particular importance to the future well-being of the Crown wards in the study. Table 5 shows a number of the dimensions that are captured in OnLAC's asset profile.
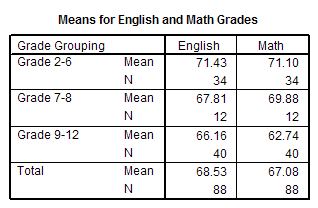
A strong correlation was found between the most recent CAFAS score for the Crown wards and the Asset Profile from OnLAC (.54). Many correlations at the .01 level of significance were found between the sub-scale scores of CAFAS and the mean scores for the time, learning, values, social, and identity variables in the Asset Profile. These correlations show that CAFAS scores improved as assets increased. In addition, it was found that both quality of access improved and the number of placements decreased as the asset profile became stronger. These correlations were significant at the .01 level of significance. As a result of the strong correlations, a regression analysis involving variables that were either highly correlated or seen as important factors in determining outcomes for the children and youth in the sample was conducted. SPSS's stepwise regression was the method of multivariate regression selected as it is suitable when a number of known variables are likely contributing to the variability of a dependent variable. We learned that 52% of the variance in the most recent CAFAS score is explained by, ranked in order of importance, the mean for the asset profile (AAR), the psychological well-being score (Kidscreen), the number of placements experienced since the last admission and gender. Frequency of access was also included in the model but again was automatically excluded by SPSS as it was not statistically significant as a predictor. Table 6 shows the means for English and math grades for the Crown wards in the sample. It was also found that the mean English mark from grades 7 through 12 was 67 as compared to the class average of 71 for students who attended the same schools as the Crown wards. The mean math mark for Crown wards in grades 7 through 12 was 64 as compared to the class average of 71.
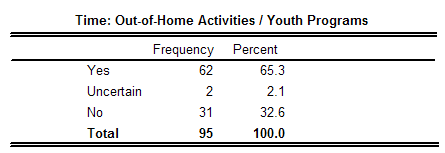
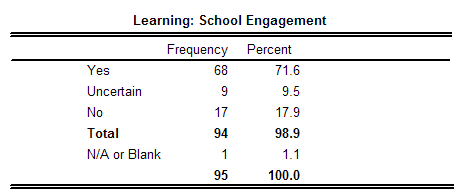
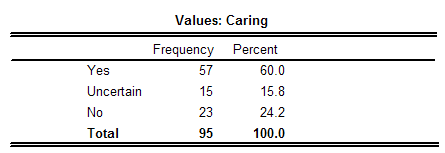
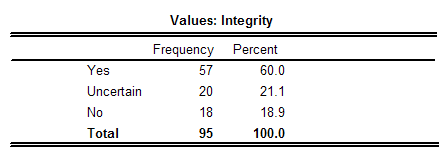
Discussion The analysis of parental service compliance found that 53% of parents either received no service or had a low level of compliance, and that 47% were in the medium and high compliance range. In order to conduct some analysis of the need for Crown wardship, the CAFAS score, ORAM and service compliance variables were considered through use of a cross tabulation. It was found that 22 children had a CAFAS score of 70 or less, came from families whose risk scores were at the mid point or less, and had parents who complied with services at the medium or high level of compliance. The chronicity of cases provided some additional information supporting Crown wardship but did not significantly explain why Crown wardship was sought in the 22 cases just described. This analysis does not provide a definitive explanation about why the children became Crown wards or about whether other alternatives might have been considered, but it does provide substantive information about why they became Crown wards. For 76% of the cases the factors examined in the study explain why Crown wardship was needed, but the results also suggest that for 24% of cases other alternatives might have been possible. Given the findings of the study, one has to ask if more effective services might significantly alter the need for Crown wardship. Renfrew County has limited services for children and families, limited public transportation, and a high rate of poverty. It would be surprising if those factors did not have an impact on children coming into the permanent care of the child protection system. How might the factors resulting in a Crown wardship decision affect the progress children make in care? The presence of addiction, caregiver mental health issues, and poor parenting were among the most prominent problems which suggests that the Crown wards were likely often exposed to inconsistent and ineffective parenting. The risk factors identified in the ORAM and entry level CAFAS scores suggest that these children and youth who became Crown wards will experience a variety of developmental issues. If we hope to succeed in helping children in care overcome their developmental deficits, we cannot be satisfied that 65% of the sample have experienced 4 or more placements. The time series CAFAS score data follow a similar pattern to a study completed by Bellamy (2007) in which males coming into care have more serious mental health and behaviour issues than females, and remain more serious than females over time. While both genders improve in their CAFAS scores over the first two years in care, they do regress over time to the original CAFAS scores found at the time of admission. The results place the females into a category that suggests they may require outpatient mental health services and the males in the middle of a category that suggests they may require more than outpatient treatment. Findings from the administration of Kidscreen indicate that females perceive their quality of life to be significantly better than do males; however, both genders are either at the mean for a normative population or not far from it in most instances. These results are encouraging, but indicating a number of areas in which improvement is needed. Farruggia (2006) demonstrated the importance and value of peer relationships, foster parent relationships, and uncovered a satisfactory level of self esteem for many in long term foster care; Kidscreen has discovered similar findings. Adair (2007), in identifying the dearth of literature on the experiences of views of children in foster care has proposed a need to develop effective instruments to carry out that kind of research. Kidscreen has shown itself to be such an instrument; it was well-received by the children and youth who completed it because they felt the questions were relevant and they liked having the opportunity to speak with someone about the quality of their lives; and it possesses sound psychometric properties supporting its ability to measure subjective well-being. The rating of the Crown wards' assets by the children's service workers indicated that the asset having to do with responsibility and the identity asset concerned with self esteem to be greatly lacking. Time spent doing out of home activities, the values of caring and integrity, the learning asset concerned with school engagement, and interpersonal skills are present for about two–thirds of the Crown wards but are an area of concern for the remaining third. Although no class averages were available for children in grades 2 to 6, it does appear that our Crown wards in that age group are doing reasonably well. The mean grades decrease as the Crown wards get older, but do not deviate greatly from their class averages with the exception of math for the grade 9 to 12 group which is substantially lower than the class average. It is possible that the deterioration in school grades and CAFAS scores in adolescence is partially explained by our Crown wards being less able to cope with the pressures of adolescence. It was worthwhile to examine the interaction of the variables within the study. CAFAS scores are strongly correlated with the number of placements experienced by the Crown wards. The strongest correlations in the study were between CAFAS scores and the various assets of the Crown wards. As assets increase the CAFAS scores improve. The findings regarding the asset profile confirm how important internal and external assets are for promoting positive outcomes for children in care. Summary 1) The children and youth are experiencing a moderate level of difficulty in their mental health and behaviour, males more so than females. 5) How the Crown wards view their quality of life portrays a more positive view about how they are doing than is evidenced in the agency's psychometric testing, and suggests that foster care is providing an environment conducive to them developing feelings of satisfaction with their lives. When these outcomes are combined with the findings about why children come into care, two considerations for future practice emerge: for those who are in care the agency's educational strategy should be maintained, and more effective strategies to improve mental health and behavior, as well as to increase assets, are required if the needs of Crown wards are to be met; better intervention strategies should be developed and implemented to attempt to reduce the number of latency-aged children and adolescents who become Crown wards, as it appears a number of them show signs of resilience and some have parents who may be capable of becoming “good enough” if offered more effective and comprehensive services. About the Author Dr. Michael O'Brien is the Director of Research and Quality Assurance at Family and Children's Services of Renfrew County and an assistant professor at Dalhousie University's School of Social Work. References Adair, F., and Duerr Berrick, J. (2007). A response to no one ever asked us: A review of children’s experiences in out-of-home care. Child and Adolescent Social Work Journal, 24(1), 23-51. Bellamy, J. L. (2007). Mental health need, outpatient service use, and outcomes among children who have experienced long-term foster care. Dissertation Abstracts International, A: The Humanities and Social Sciences, 67(10), pp. 3978. Blome, W.W. (1997). What happens to foster kids: Educational experiences of a random sample of foster care youth and a matched group of non-foster care youth. Child and Adolescent Social Work Journal, 14(1), 41-53. Buehler, C., Orme, J. G., Post, J., and Patterson, D. A. (2000). The long term correlates of family foster care. Children and Youth Services Review, 22, 595-625. Cook-Fong, S. K. (2000). The adult well being of individuals reared in family foster care placement. Child Youth Care Forum 29, 7-25. Farruggia, S. P., Greenberger, E., Chen, C., and Heckhausen, J. (2006). Perceived social environment and adolescents’ well-being and adjustment: Comparing a foster care sample with a matched sample. Journal of Youth and Adolescence, 35(3), 349-358. Flynn, R. J., Ghazal, H., and Legault, L. (2006). Looking After Children: Good Parenting, Good Outcomes. Assessment and Action Records. (Second Canadian adaptation, AAR-C2). Ottawa, ON, and London, UK: Centre for Research on Community Services, University of Ottawa and Her Majesty’s Stationery Office (HMSO). Hodges, K. (1999). Child and adolescent functional assessment scale. In Maruish, M. (ed). The Use of Psychological Testing for Treatment Planning and Outcome Assessment. Mahwah, N.J.: Lawrence Erlbaum Associates Inc. Leathers, S. J. (2006). Placement disruption and negative placement outcomes among adolescents in long-term foster care: The role of behavior problems. Child Abuse & Neglect, 30(3), 307-324. Marquis, R., and Flynn, R. (2008). Mental health of young people in care: Comparing Canadian foster youth with British and American general population youth. Ontario Association of Children’s Aid Societies Journal, 52(4), 2-6. McDonald, T. P., Allen, R. I., Westerfelt, A., and Piliavin, I. (1996). Assessing the Long Term Effects of Foster Care. Washington, D.C.: CWLA Press. OACAS (1997). The Eligibility Spectrum. Toronto, ON: Ontario Association of Children’s Aid Societies. OACAS. (2000). Ontario Risk Assessment Model. Toronto, ON: Ontario Association of Children’s Aid Societies. Orangewood Children’s Foundation. (2001). Fact sheet. Orange, CA: Orangewood Children’s Foundation. Ravens-Sieberer, U. (2006). The Kidscreen questionnaires, Berlin, Germany: Pabst Science Publishers. Trout, A. L., Hagaman, J., Casey, K., Reid, R., and Epstein, M. (2008). The academic status of children and youth in out-of-home care: A review of the literature. Children and Youth Services Review, 30, 979-994. Previous article: Message from the Executive Director Next article: SUCCESS! Play Life to Win |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Download PDF version. To change your subscription or obtain print copies contact 416-987-3675 or webadmin@oacas.org |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}